Perimenopause Is Not an Oestrogen Deficiency
For years, perimenopause has been framed as a slow decline in oestrogen.
Lower hormones.
Lower function.
Replace what’s missing.
But emerging research is telling a far more nuanced and clinically relevant story.
In the early years of perimenopause, the issue is often not low oestrogen at all.
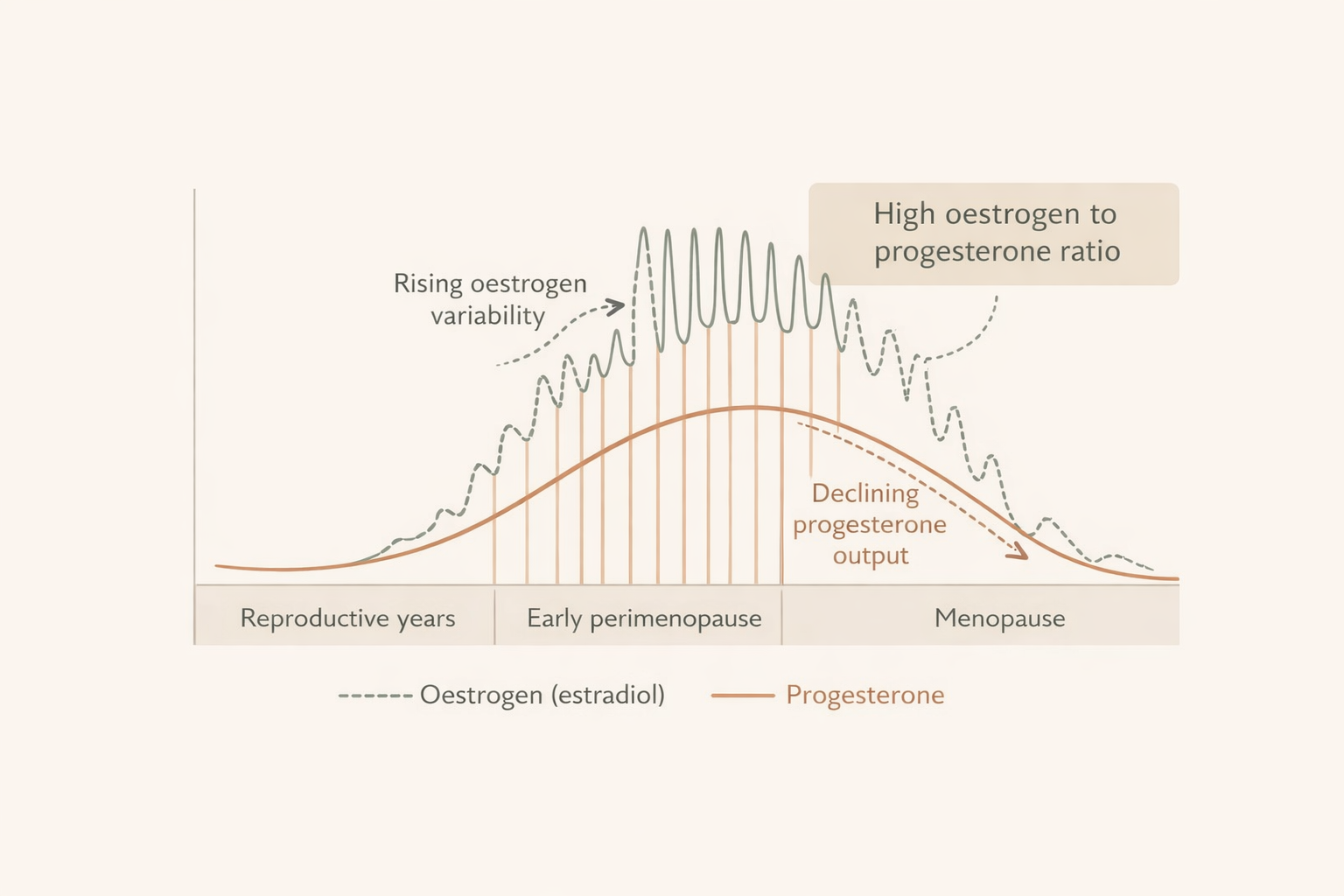
It’s high and erratic oestrogen alongside falling progesterone.
And that hormonal ratio matters profoundly for the brain, metabolism, inflammation, and how women feel in their bodies.
This shift helps explain why so many women in their late 30s and early 40s experience:
• anxiety and low mood
• poor sleep
• memory changes and brain fog
• heavier or more painful cycles
• migraines
• worsening PMS
• sudden intolerance to stress
—even while their blood tests are labelled “normal”.
What Actually Happens in Early Perimenopause
Ovulation becomes less consistent long before periods stop.
And when ovulation falters, progesterone production drops first.
Oestrogen, however, doesn’t gently decline.
It often becomes higher, spikier, and more unpredictable.
This creates a state of:
High oestrogen exposure relative to low progesterone.
Clinically, this is often referred to as an oestrogen-dominant pattern—though in reality it’s more accurately a progesterone-deficient imbalance state.
Your cycle may still appear regular.
Your hormones may sit within reference ranges.
But the internal signalling environment has changed.
New Research: It’s The Ratio That Matters
A recent animal study published in Nature Communications explores how this imbalance occurring in early perimenopause is not low oestrogen, but high oestrogen paired with low progesterone, and may even contribute to long-term neurological risk.
The results were striking.
When the oestrogen-to-progesterone ratio was elevated:
• brain metabolism declined
• memory worsened
• neurological stress increased
When progesterone alone was restored — without adding more oestrogen — brain function improved.
This strongly suggests that many early perimenopausal symptoms are being driven by hormonal imbalance, not deficiency.
Why Progesterone Matters So Much
Progesterone isn’t just a “cycle hormone”.
It plays critical roles in:
• calming the nervous system
• supporting sleep architecture
• modulating inflammation
• protecting brain tissue
• balancing oestrogen signalling
When progesterone drops:
Oestrogen’s stimulating effects become unopposed.
This can amplify:
• anxiety and irritability
• poor stress tolerance
• heavy or painful bleeding
• headaches and breast tenderness
• sleep disruption
Many women are told they’re “too young for perimenopause”.
Physiologically, their hormone patterns often tell a different story.
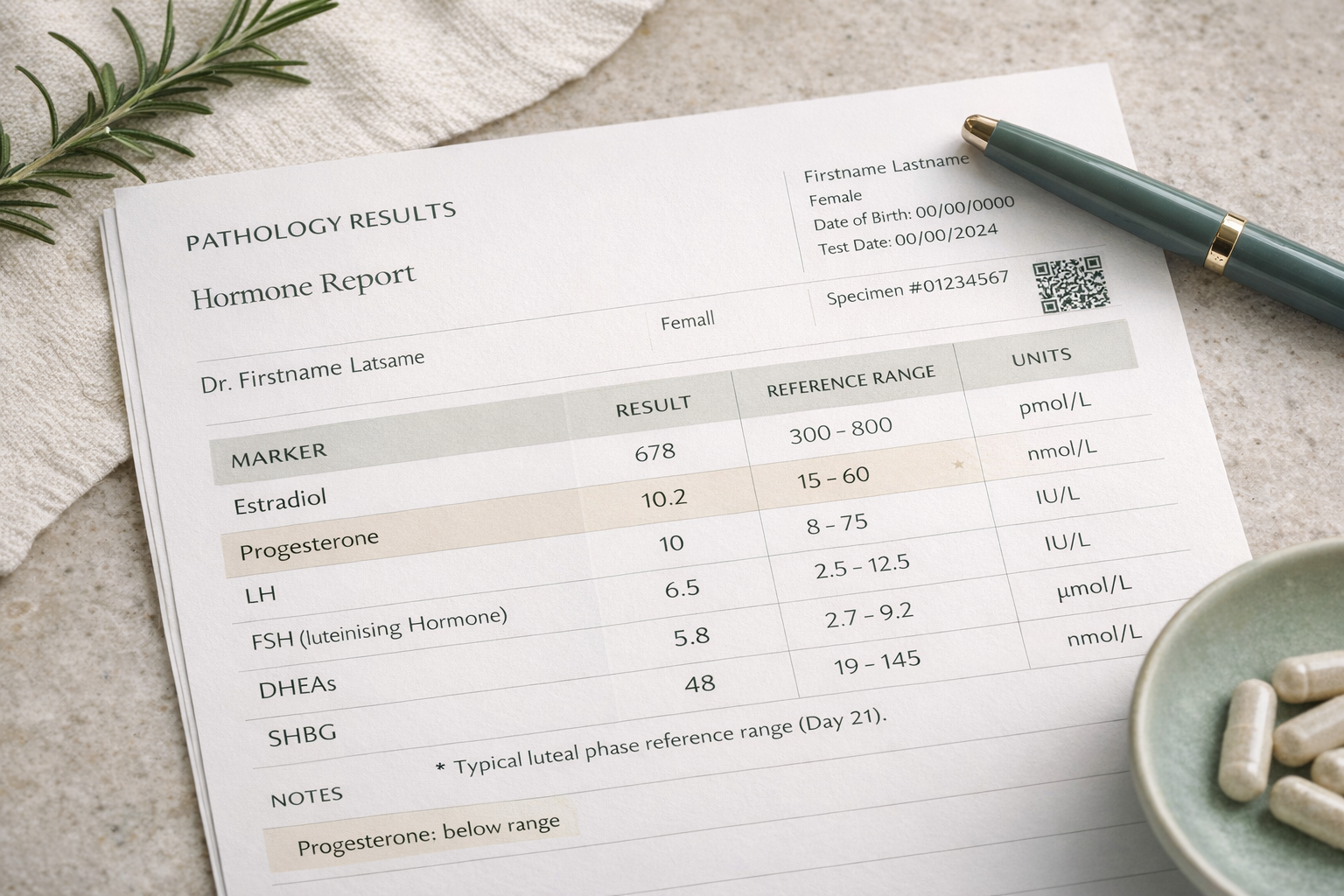
Why Standard Testing So Often Misses This
Most conventional hormone testing looks at isolated values.
One snapshot.
One reference range.
But hormonal health is about:
• patterns across the cycle
• ratios between hormones
• ovulation quality
• stress-hormone interaction
• liver and gut clearance
A woman can have:
“Normal” oestrogen
“Normal” progesterone
And still be experiencing a profound imbalance state.
This is why so many women feel dismissed, and why symptoms are often attributed purely to stress, anxiety, or ageing.
How Novara Approaches Perimenopause Differently
At Novara, we don’t treat hormones as standalone numbers.
We assess perimenopause as a whole-system transition involving:
• ovulatory function
• oestrogen-progesterone dynamics
• cortisol and nervous system load
• inflammation
• metabolic shifts
• gut–liver hormone clearance
• nutrient status
Because hormone symptoms don’t occur in isolation.
They emerge from how systems interact.
Our process is structured, testing-informed, and personalised—allowing us to identify:
• whether symptoms are driven by imbalance vs deficiency
• how stress physiology is influencing cycles
• where hormone metabolism may be impaired
• what support will actually restore regulation
Rather than simply suppressing symptoms or defaulting to blanket hormone replacement.